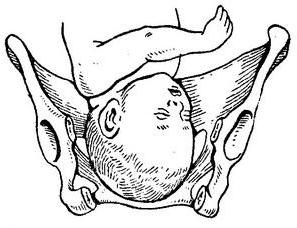
During childbirth, the fetus passes to the exit from the birth canal, performing translational and rotational movements. The complex of such movements is a biomechanism of labor. Presentation of the fetus largely determines the complexity of childbirth. More than 90% of cases are occipital presentation of the fetus.
Primogenous biomechanism
According to studies, in primiparas, the head progresses slightly during pregnancy. The degree of this progression depends on the ratio of the size of the fetal head and the mother's pelvis. For some, the fetus stops its movement in the entrance, and for some, it is already in the expanded part of the
pelvic cavity
. When childbirth begins, the head resumes its advancement when the first contractions appear. If the birth canal is obstructed, the biomechanism of labor in the anterior view of the occipital presentation occurs in the pelvic area where the obstruction is encountered. If childbirth proceeds normally, then the biomechanism turns on when the head passes the boundary between the wide and narrow parts of the pelvic cavity. To cope with the obstacles that have arisen, only uterine contractions are not enough. Attempts appear, pushing the fetus along the way to exit the birth canal.
In most cases, the biomechanism of childbirth with the front view of the occipital previa is activated at the stage of expulsion, when the head passes into the narrow part of the pelvic cavity from the wide, although in primiparous everything can begin at the time of opening, when the fetal head is in the entrance.
During the process of expelling the fetus, the fetus and the uterus constantly interact with each other. The fetus tries to stretch the uterus in accordance with its shape and size, while the uterus tightly covers the fetus and amniotic fluid, adapting it to its shape. As a result of such actions, the fetal egg and the entire birth canal achieve the most complete correspondence to each other. So there are prerequisites for the expulsion of the fetus from the birth canal.
Division into moments
The biomechanism of childbirth with the front view of the occipital presentation is conditionally divided into four points:
- head bending;
- its inner turn;
- extension of the head;
- internal torso rotation in combination with an external rotation of the head.
First moment
Bending the head consists in the fact that under the influence of intrauterine pressure, the cervical spine bends, bringing the chin closer to the chest, and lowering the back of the head. At the same time, the small fontanel is located below the large, gradually approaching the wireline of the pelvis, and this part becomes the lower part of the head.
The advantage of such bending is that it gives the head the ability to overcome the cavity of the small pelvis with the smallest size. The direct size of the head is 12 cm, and the small oblique resulting from bending is 9.5 cm. However, with the normal course of labor, there is no need for such a strong bending of the head: it bends as much as necessary to pass from wide to narrow part of the pelvic cavity. Maximum bending of the fetal head is only required in situations where the width of the birth canal is not enough to pass the head. This happens when the pelvis is too narrow, as well as in the case of posterior view of the occipital presentation.
Flexion is not the only fetal movement at this point in the biomechanism of labor. At the same moment, the head moves forward along the birth canal, and after the end of bending, its internal rotation begins. So at the first moment of the biomechanism of childbirth, there is a combination of translational motion with flexion and rotational. However, since the most pronounced movement is the bending of the head, the name of the first moment reflects this fact.
Second moment
An internal rotation of a head is a combination of its translational motion with an internal rotation. It begins when the head is bent and set at the entrance to the small pelvis.
The fetal head, moving progressively in the pelvic cavity, encounters resistance to further movement and begins to turn around the longitudinal axis. As if screwing the head into the pelvis. This occurs most often when it passes from a wide to a narrow section of the pelvic cavity. The nape glides along the wall of the pelvis, approaching the pubic joint. This moment can be fixed by monitoring how the position of the swept seam changes. This seam before the turn is in the small basin in the transverse or oblique size, and after the turn is located in the direct size. The end of the head rotation is noted when the sagittal suture is installed in direct size, and the suboccipital fossa assumes a position under the pubic arch.
Third moment
Extension of the head. The head continues to move along the birth canal, beginning to gradually expand. In normal childbirth, extension is performed at the exit of the pelvis. The nape comes out from under the pubic arch, and the forehead protrudes beyond the tailbone, protruding the back and front of the perineum in the form of a dome.
The suboccipital fossa rests on the lower edge of the pubic arch. If at first the extension of the head was slow, at this stage it accelerates: the head extends literally in a few attempts. The head penetrates through the vulvar ring in its small oblique size.
In the process of extension from the birth canal, the crown, frontal region, face and chin appear in turn.
Fourth moment
External rotation of the head with internal rotation of the body. While the head follows along the soft tissues of the pelvic outlet, the shoulders are screwed into the pelvic canal. The energy of this turn gets the born head. At this moment, the back of the head turns to one of the hips of the mother. The anterior shoulder is the first to leave, followed by a slight delay due to the folding of the tailbone, and the posterior shoulder is also born.
The birth of the head and shoulders sufficiently prepares the birth canal for the appearance of the rest of the body. Therefore, this stage is quite easy.
The considered biomechanism of childbirth in the anterior view of the occipital presentation for the primiparous is completely correct for the multiparous. The only difference is that in those giving birth again, the onset of the biomechanism falls on the period of exile, when the waters flowed away.
Obstetrician Activities
In addition to biomechanism, it is necessary to use obstetric benefits in childbirth.
Not everything can rely on nature. Even if the woman in labor has a relatively regular birth in the occipital presentation, the help of an obstetrician may be needed.
- First moment. Protection of the perineum, preventing extension early. With palms, you need to hold the head, obstructing movement during the effort and increasing bending. It is necessary to strive to ensure that bending is not maximum, but one that is genetically necessary. Without extreme necessity, no need to intervene. The child is usually able to adapt to the birth canal. Many obstetric benefits in childbirth, and not the birth itself, cause many complications and birth injuries . More often the child is injured not from the crotch of the woman in labor, but from the hands of the midwife protecting the crotch.
- The second point - in the absence of attempts to remove the head from the genital gap. If the head comes out at maximum effort, it strongly presses on the sexual gap.
The order is as follows. With the completion of the attempt, the vulvar ring is gently stretched with the fingers of the right hand over the emerging head. Stretching is interrupted with the start of a new attempt.
These actions, aimed at obstetric allowance, must be alternated until the head approaches the parietal tubercles to the genital opening, when head compression increases and the perineum stretches. As a result, the risk of injuries to the fetal head and the woman in labor is increased.
The third point is to minimize crotch tension to increase the flexibility of the piercing head. The obstetrician gently presses the fingertips on the tissues surrounding the genital opening, directs them towards the perineum, which makes it less stressful.
The fourth point is the adjustment of attempts. The appearance of the parietal tubercles of the head in the genital fissure carries an increased risk of rupture of the perineum and traumatic compression of the head.
Equally great danger is the complete cessation of attempts. An important role in this is respiration. A woman in labor is told to breathe deeply and often with her mouth open to ease the attempts. When a need arises in a push, a woman in labor is forced to push a little. By the method of initialization and termination of attempts, the midwife controls the birth of the head at the most critical time.
The fifth point is the appearance of the shoulders and torso. After the head is released, the woman in labor must push. Hangers are usually born without the help of an obstetrician. If this does not happen, the head is gripped by hands. The palms of the hands touch the temporal-buccal areas of the fetus. The head is first pulled down until one of the shoulders appears under the pubic arch.
Then, with the left hand, the head is taken and lifted up, and with the right hand, the crotch moves from the back shoulder, which is neatly displayed. Having liberated the shoulder part, the body is lifted up behind the armpits.
In a number of cases, to prevent intracranial injury, a perineotomy is performed if the perineum is intractable.
Complications
Although childbirth with the front view of the occipital presentation regularly demonstrates the biomechanism, complications can also occur. Strongly affects the possibility of safe delivery of the size of the pelvis. Complex births occur if the woman in labor has a narrow pelvis. This pathology is quite rare. It serves as the reason for the decision to have a planned caesarean section. There are other adverse factors that can complicate childbirth: a large or postponed fetus. In these cases, a planned caesarean section is often chosen . In some cases, the need for the end of childbirth through a cesarean section appears only in their course.