In surgery, two concepts are distinguished - tracheotomy and tracheostomy.
Tracheotomy is the opening of the trachea and the insertion of a tube into it to allow air to enter the lower respiratory tract during asphyxiation. This is an emergency operation.
A tracheostomy is also an opening of the trachea, but with the hemming of the edges of the resulting incision to the underlying tissues and the formation of an opening for breathing.
A bit of history
This method of emergency care was known in ancient Egypt and India, there is documentary evidence that even Alexander the Great used it to save soldiers in his army. Hippocrates and Gallen wrote about this procedure, but because of its invasiveness and danger to life, they were not recommended to use it often in practice.
The first successful operation was performed by the Italian physician Anthony Brasavol in 1546. This is the first documented evidence that the patient remained alive after the manipulation. Since 1718, this type of surgical intervention has become ordinary and has been used more widely by doctors. Nevertheless, many were still afraid to use it. For example, George Washington’s personal physician preferred his patient to die than dare to perform risky manipulations.
The advent of the rules of aseptic and antiseptic somewhat reduced the risk of complications and mortality, but still did not convince the medical community that this method is safe for the patient. Currently, tracheotomy is an emergency way of help, which is used only when all other methods (Heimlich's reception, intubation) are ineffective or there is no time for them.
Indications for surgery
No matter how simple the tracheotomy may seem, the indications for it are quite strict, since the risk to a person’s life during this manipulation exceeds the possible benefit. It:
- Foreign bodies located above the trachea, which cannot be removed by other means.
- Closed injuries narrowing the lumen of the larynx.
- Acute stenosis of the larynx with diphtheria croup, whooping cough, measles, typhus, etc.
- Overlap of the lumen of the trachea or larynx with a tumor.
- Compression of the upper respiratory tract from the outside.
- Chemical burns
- Allergic stenosis.
Types of airway obstruction
- Acute, or lightning-fast, develops in just a few seconds. It can be like blockage by foreign bodies, as well as allergic edema.
- Acute - manifests itself in a matter of minutes, usually associated with diphtheria or foreign bodies.
- Subacute - closure of the lumen of the respiratory tract can last tens of minutes, or even hours. This condition is typical for false croup, sore throat, chemical burns.
- Chronic - can grow over the years with pathological processes such as laryngeal cancer, perichondritis, cicatricial narrowing of the trachea.
Classification
There are several types of tracheotomy, depending on the technique.
Dissection Level:
- Upper: at the level of the cricoid cartilage.
- Medium: at the level of the thyroid cartilage.
- Lower, or conicotomy.
The nature of the section distinguish:
- Longitudinal.
- Transverse.
- U-shaped.
Instruments
Do not forget that for all its urgency and improvisation, this technique is positioned as an operation. A tracheotomy should be performed with a specific set of instruments, if any. Conventionally, they can be divided into two large groups: these are general surgical instruments and specialized ones.
The first group includes tweezers, a scalpel, clamps for stopping blood, surgical scissors, hooks for diluting tissues, a catheter, syringes and needles. The second group includes the Luer tracheotomy cannula, consisting of two tubes located one in the other; Chassignac hook designed to hold the trachea without traumatizing it; trachea expander and hook to move the isthmus of the thyroid gland.
Technique for performing tracheotomy
Before any operation, appropriate preparation is carried out, which helps the doctor as quickly and as painlessly as possible for the patient to carry out the necessary intervention. In this case, it is necessary to put the patient on his back and throw his head back as far as possible so that the tracheal cartilage is clearly visible. For this, a roller is sometimes used. After fixation, the person receives anesthesia. It can be either general inhalation or local. It all depends on the conditions in which the operation is performed, the age of the patient, the capabilities of the doctor and the hospital. If the situation is urgent, then the doctor performs the manipulation without anesthesia. After all preparations, a tracheotomy begins directly.
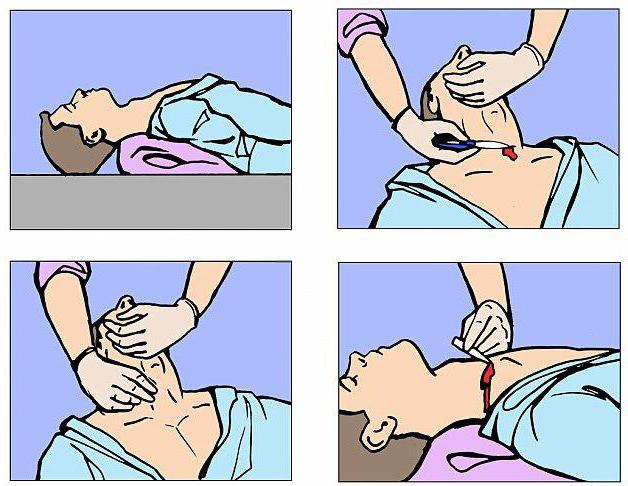
The technique consists in a layered incision of the skin, subcutaneous fat, fascia and fibrous membrane downward from the thyroid cartilage. Then the muscle is exposed, which in a blunt way is bred to the sides. Under it is the cartilage and the isthmus of the thyroid gland. The gland is separated from the trachea and pushed up, another fascia is dissected. The larynx is fixed with a hook and, limiting the scalpel blade with a finger, bandage or adhesive, a small incision is made. The goal is achieved. The air again enters the lungs. At first, respiratory arrest may occur, but then the patient begins to cough and turn pink. Only after the doctor has made sure that the person has started breathing again, cannula is inserted into the wound and fixed with sutures or plaster. The wound is sutured so that it holds the tube tightly.
Conicotomy
This is a small operation preceding a tracheotomy, if there is no possibility and time to conduct a tracheotomy normally. Performing it, no longer make phased cuts. One movement dissects the neck up to the cricoid cartilage and the thyroid cricoid ligament. A clip is inserted into the incision, its branches are bred and they are fixed in this position. If the patient began to breathe, turned pink, he developed a cough, then the procedure was successful. Once the danger has passed, the conicotomy can be converted into a tracheostomy to ensure a constant flow of air for the patient.
Possible errors during the manipulation
Any operation has its consequences; tracheotomy is no exception. Complications that arise in connection with it can be divided into three groups.
- During the operation:
- an incorrect incision line can cause venous bleeding, air embolism, and sometimes transection of the common carotid artery ;
- blood can enter the lower respiratory tract, causing repeated asphyxiation;
- the incision should be equal to the diameter of the cannula, otherwise it will have to be sutured and injured the tissue even more;
- a deep cut can cause injury to the esophagus, so the scalpel blade must be limited to 1 cm.
2. Immediately after surgery:
- hypoxia;
- fracture of the tracheal ring or its puncture;
- subcutaneous emphysema;
- pneumothorax.
3. Delayed consequences:
- tracheobronchitis;
- stenosis of the trachea and repeated asphyxia;
- change (hoarseness) of the voice due to transection of the recurrent nerve;
- cosmetic defects.
All doctors from a student's bench remember how dangerous a tracheotomy is. This is not an operation that can be performed continuously. Only in emergency, special cases, when the patient is on the verge of life and death, as in a hurry you can harm the patient. And if this manipulation is not carried out in a hospital, but somewhere on the street or at home, then it’s worth a hundred times to think before deciding. Simple at first glance, the technique should be supported by sufficient experience of the surgeon. A tracheotomy at home is not just impossible, it is dangerous. If you do not have a medical education and relevant skills, do not try to repeat it.
A tracheotomy is advisable only to save a person’s life! The risk of death or serious complications is high enough to make the doctor think about alternatives. Even considering the fact that this operation has been known since time immemorial, the medical community has not yet figured out how to make it safe enough.
A tracheotomy is an opportunity to save someone's life, but at the same time the same equivalent opportunity to take it away.