The shoulder joint, the anatomy of which is discussed in the following article, allows the arms to move freely. Ligaments, in contrast, limit mobility.
Let us examine in detail what the shoulder joint is, the topographic anatomy of which is represented by the mutual arrangement of tissues, nerves and blood vessels.
In the shoulder girdle, the joints combine the clavicle and sternum with the scapula, due to which acromioclavicular and sternoclavicular joints are formed. Let's start in order.
Bones
The anatomy of the human shoulder joint is complex. To provide mobility, the depression here is less conceived, and the range of motion is provided by many tendons and muscles.
The joint consists of two large bones - the humerus and scapula, several joints and many ligaments, tendons and muscles.
The shoulder blade is a flat bone in the form of a triangle. It is also important when building the joint of the shoulder joint. The bone is located on the back of the body and is easily felt under the skin. There is a joint cavity on it, to which the humerus is attached.
On the back of the scapula there is an axis dividing it in two, where the infraspinatus and supraspinatus muscles are located.
On the scapula there is another process, called the coracoid, attaching ligaments and muscles. Another bone - the clavicle - is tubular, with a curved shape.
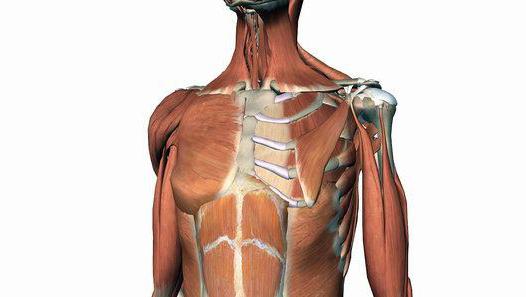
The entire shoulder joint (anatomy) of the photo below illustrates.
Muscle
The rotational or rotator cuff is one of the most important joints of the muscles in this part. The muscles help bring, flexion and extension of the arm.
Injuries in this area are most often associated with the cuff. Athletes put themselves at particular risk. However, troubles also occur in everyday life, especially when they lift weights and carry the load without distributing the weight correctly. If the muscles are damaged, the anatomy of the shoulder joint is impaired. Muscles then can not promote movement as before, and the amplitude is sharply reduced.
So, the cuff consists of:
- supraspinatus;
- papillary small round;
- subscapularis muscle.
Blood supply and innervation
The muscles of the shoulder girdle receive blood due to the axillary artery and its branches. It crosses the armpit cavity and moves from the first rib to the bottom of the pectoralis major muscle, passing into the brachial artery. She is accompanied by a vein.
Innervation is realized through the nerves of the brachial plexus. Both spinal and those coming from the anterior branch of the thoracic nerve take part in it. The brachial plexus originates from the base of the neck, moves forward and down, penetrating into the armpit cavity, goes under the clavicle, under the coracoid process of the scapula, giving off nerves there.
What causes the movement?
The shoulder joint can move due to the following five joints (three joints and two joints of the muscular-tendon plan):
- Shoulder-shoulder joint.
- Bag education.
- Moving the scapula across the chest.
- Acromioclavicular joint.
- Sternum-clavicular joint.
Look at the photo. Here is the shoulder joint: structure, anatomy. The complex structure of this area is best understood for understanding, analyzing the image.
In order to ensure full movement, all five joints must work smoothly and correctly. Any violation cannot be replaced by other joints. This is why pain and movement restriction always accompany damage to this area.
Acromioclavicular joint
The anatomy of the shoulder joint is characterized by multiaxiality and flatness, due to which the clavicle merges with the scapula. It is held by a strong coraco-clavicular ligament, directed from the coracoid process of the scapula to the bottom of the clavicle. The shoulder blade is able to rotate around the sagittal axis, which passes through the joint, and also move slightly around the transverse and vertical axes. It turns out that movements in this joint can be made around 3 axes. Nevertheless, the amplitude here is very small.
Sternum-clavicle
The anatomy of the shoulder joint is also presented multiaxially and flatly. The surface consists of the sternum of the clavicle and the clavicular notch of the sternum. The shape of the surface of the joints resembles a saddle. Between them is a disk that fuses with the capsule and divides the joint cavity in two. A thin capsule is attached by ligaments woven into the fibrous membrane on both sides. In addition, there is an interclavicular ligament that connects the sternal ends of the clavicle, as well as the costoclavicular, located in the lateral position at a small distance from the joint.
The anatomy of the shoulder joint is represented by three axes. It has a fairly limited amplitude. Therefore, they can be moved forward, backward and slightly rotated. Circular motion may occur when the end of the collarbone makes an ellipse.
Scapula ligaments
In addition to the joints, there are fibrous bundles on the belt of the upper extremities - this is the ligament of the scapula. They consist of lower and upper transverse, as well as coracoid-acromial. The latter is presented in the form of a triangle, where the arch is stretched over the shoulder joint between the coracoid process and the apex of the acromion. The ligament serves as a protection for the shoulder joint and, together with others, limits mobility during shoulder abduction. The lower transverse is located between the edge of the articular cavity of the scapula and the base of the process of the shoulder, and the upper transverse ligament is thrown through the scapular notch.
The structure and ligaments of the shoulder joint
In the free part of the limb, the joints are merged between themselves and the belt of the upper limb, due to which the wrist, elbow, shoulder and other areas are formed.
The shoulder joint has a multiaxial and spherical structure. It consists of the head of the bone and the cavity of the scapula. The surface of the first is spherical, and the second has the form of a fossa. The head is about three times the cavity that the lip of the joint supplements. The latter somewhat increases its surface, adding depth, curvature and congruence.
The capsule of the joint is large but thin. It originates at the lip and is attached to the neck of the humerus. Inside the capsule spreads between the tubercles of the humerus and forms the inter-tubercle synovial vagina. The capsule is fixed by the coraco-brachial ligament directed from the process of the scapula and interwoven into it.
Movement features
In the ligament of the shoulder joint, the anatomy is characterized by underdevelopment. Due to the considerable difference between the contacting surfaces in the shoulder joint, a large amplitude of movement with respect to the three axes is possible: vertical, sagittal and transverse. Around the sagittal shoulder is retracted and driven, around the transverse - it bends and unbends, and the vertical one - turns in and out.
In addition, the anatomy of the shoulder joint allows for circular movements. They in this area can occur together with the belt of the upper limb. As a result, it is able to describe a hemisphere to a greater or lesser extent. But leading her above the horizontal level stops a large tubercle of the humerus.
You need to know that the abduction of the hand, due to the work of only the humerus and the articular cavity, is brought only to ninety degrees. Then the scapula begins to help the movement, due to which the abduction increases to 180 degrees.
Not only problems in the muscles and tendons of this area lead to destabilization of the state of the upper limb. They can be caused by chest deformities or spinal disorders. Therefore, it is so important to be careful about your health and pay attention to the symptoms that arise in a timely manner. Then it will be possible to maintain health and full movement for life.
Diseases and anatomy of the shoulder joint, MRI
For shoulder pain, it is imperative to consult a specialist so that he makes the correct diagnosis. The condition of the bones will help to find out the x-ray. Soft tissues and cartilage are examined after ultrasound. An excellent and safe way is MRI. The anatomy of the shoulder joint can also be viewed with arthroscopy, which, in addition to diagnosis, also treats the patient.
Consider the most common diseases.
Bursitis
The disease is diagnosed with inflammation of the inversion of the synovial bag of the shoulder joint. The anatomy in this part is very complex. The lesion usually occurs between the bone and the tendon. A feature of bursitis of the shoulder joint is that the synovial bag here does not communicate with its cavity.
The causes of bursitis can be both injuries and infections, as well as excessive loads on the joint in athletes and workers engaged in heavy physical labor.
Periarthrosis of the shoulder blade or periarthritis
It is also a common condition for pain in the shoulder area. This includes a whole group of the following diseases.
- Osteochondrosis develops in the cervical spine. The pain spreads through the nerves and passes into the brachial plexus. Then the so-called plexitis develops. The treatment method is selected depending on the condition of the nerve endings, as well as the intervertebral discs.
- Subacromial impingement syndrome is characterized by squeezing of the shoulder rotators that pass between the head of the shoulder and the process of the scapula. The channel may be crushed or injured. Then the person will feel pain, especially at night. He will not be able to lie on his shoulder, bend his arm and take her aside. During treatment, anti-inflammatory drugs are selected, and physiotherapy is also prescribed. Ointments, massages, compresses and gymnastics are used. If necessary, a surgical operation is also prescribed.
- Cuff rupture occurs as a result of injury, squeezing, or stretching. The tendon is rubbed. The shoulder starts to hurt, and the pain gives in the arm, because of which it can be impossible to bend and take away. At rupture, surgery is required where the tendons are sutured by arthroscopy. In this case, the main thing is not to miss the optimal time, the result will be better the sooner the problem is clarified and eliminated.
- When the joint capsule sticks together during inflammation, an adhesive capsulitis is diagnosed. The patient is less able to move his hand. If arthroscopic surgery is not performed, then in the future the only option for regaining mobility will be prosthetics.
- Due to chronic stretching of the muscle and tendon under the scapula, as well as trauma, the “frozen shoulder” syndrome develops. At the same time, pain and limitation or inability to take the arm outward are felt. To relieve the patient from suffering, the affected area is punctured with an anesthetic.
- Due to trauma, the cartilaginous lip may be damaged and it may rupture. Recovery is possible with arthroscopy.
Prosthetics
To replace the surfaces damaged by trauma or illness, the shoulder joint is prosthetically. The anatomy of the articular cavity remains unaffected. An artificial implant is installed only in cases where other methods of treatment are ineffective.
So, it becomes the only solution after the fracture, when the anatomy of the shoulder joint and shoulder muscles cannot be restored and the metal retainer was useless.
Prosthetics will also be required at the advanced stage of osteoarthrosis. Cartilage damage is accompanied by pain, crunching and limited movement. Patients become helpless. At the same time, prosthetics restores the work of the hands, and the person gets rid of the pain.
The same goes for muscle damage to the rotator cuff. If at the beginning of the disease arthroscopy will be an effective treatment method, then later, in the neglected version, it will be powerless. Therefore, an implant is installed.
A severe form of a disease such as rheumatoid arthritis is also dangerous. The surfaces of the joint are destroyed, the muscles of the rotational cuff and other soft tissues are damaged, severe pain is felt, and movement is limited and gradually leads to immobilization.
Whatever manipulations on the joint are carried out, after them the hand is necessarily fixed with an orthosis, bandage or bandage. In order for the functioning of the upper limb to return to normal, a comprehensive treatment is carried out, implying various recovery measures. These include special training, massage and physiotherapy.