Rectal resection is the excision of its affected part. The rectum continues the colon and is located from the sigmoid to the anus. This is the final part of the digestive tract, the length of which is 13-15 cm. Fecal masses accumulate in it and subsequently are brought out. It got its name because it has no bends. The main ailments of the rectum are: various processes of inflammation, Crohn's disease, obstruction, ischemia, cancer. The main treatment for such diseases is surgery.
Types of operations
For the elimination of colorectal cancer, the best treatment is surgery. In medical practice, there are, depending on the location of the tumor and its size, several techniques for its excision:
- Polypectomy is the simplest operation to remove polyps and minor tumors. When it is carried out, nearby tissues are minimally damaged. Surgery is performed using an endoscope if the neoplasm is located next to the anus.
- Front resection of the rectum - is done by removing its upper part and the lower end of the sigmoid colon. The rest of it is connected to the sigmoid colon. At the same time, the nervous apparatus and anus are preserved. For quick healing, a temporary colostomy is sometimes applied, which is removed after a second operation after about two months.
- Low anterior resection - performed when the pathology is removed in the middle part of the rectum. In this case, the damaged part of the sigmoid and the entire rectum, except the anus, is excised. The bowel function is lost. A place for the accumulation of feces is formed from the reduced intestine, which is located above. The sigmoid colon is connected with a direct anamostosis. In almost all cases, a stoma is placed for unloading within a few months.
- Abdominal-anal resection - performed from the abdominal cavity and anus. Rectal resection is done when the pathology is located close to the anus, but does not affect it. The part of the sigmoid colon that is completely straight with the share of the anal sphincter is subject to removal. The remaining sigmoid colon is used to form an anastomosis with part of the anal sphincter.
- Abdominal-intermediate extirpation - through two incisions, one of which is on the stomach, and the other around the anal canal. In this case, the rectum, anal canal and muscles of the anal sphincter are subject to resection. Feces are discharged through the formed stoma.
Resection Technique
The operation to remove part of the rectum can be performed in two ways: using laparotomy or laparoscopy. With laparotomy, an incision is made along the lower abdomen. The surgeon gets a good overview for all the manipulations. The laparoscopic method involves several small holes for the introduction of surgical instruments into the abdominal cavity. The technique of open-ended rectal resection is as follows:
- The surgical field is treated and an abdominal wall incision is made. The abdominal cavity is carefully examined and the affected area is located.
- This area is isolated by clamping and removed to healthy tissue. At the same time, a part of the mesentery with vessels feeding the intestine is excised. Before removal, the vessels are ligated.
- After excision of the neoplasm, the ends of the intestine are sutured, and it can function again.
When moving from one stage of the operation to another, the surgeon makes a change of instruments to avoid infection with intestinal contents.
Laparoscopic anterior rectum resection
As mentioned earlier, resection can be performed not only in an open way, but also with the help of laparoscopy. In this case, several holes are made into which laparoscopic instruments are inserted. The proven methodology for conducting such operations is becoming increasingly popular due to the low morbidity of the patient and a number of other advantages. The operation of the anterior resection of the rectum in the upper sections begins with the intersection of blood vessels. Then, the affected part of the intestine is secreted and excreted through a small hole in the anterior abdominal wall, where a resection is made, and the ends of the intestine are sutured.

The same steps are performed during resection of the lower colon. Anastomosis (the connection of two parts of the intestine) is carried out based on the anatomical conditions. With a sufficient loop length, the area with the tumor through the hole is brought out, its excision is made, the ends are sutured. Otherwise, when the length of the intestine does not allow to bring it out, the resection and connection of the ends is performed in the abdominal cavity, using a special circular stapler.
The benefits of laparoscopic surgery
It has been experimentally established that the results of operations performed by the laparoscopic method are not inferior in quality to the results of rectum resection performed using laparotomy (open access). In addition, they have the following advantages:
- less injuries;
- short term rehabilitation and recovery of the patient after surgery;
- minor pain symptom;
- lack of suppuration and postoperative hernia;
- a small percentage of complications in the initial and long-term period.
Laparoscopy Disadvantages
The disadvantages include:
- The method of laparoscopy is technically not always possible. It is safer for the patient to perform open access surgery.
- Resection requires expensive tools and equipment.
- The operation has its own specifics and is performed by highly qualified specialists, the training of which requires certain funds.
In some cases, during the operation, which is started by laparoscopy, they switch to laparotomy.
What will happen after the operation?
After resection of the rectum, the patient is transferred to the intensive care unit, where he will recover from anesthesia. Then the patient is placed in the ward of the Department of Surgery for further rehabilitation. In the first time after the surgical period, the patient is given intravenous nutrition using a dropper. Seven days later, it is allowed to switch to the use of ordinary food prepared in liquid form. Gradually, the transfer to solid food is carried out. For a quick recovery, motor activity has a great influence, so the patient is recommended to walk and perform exercises for the respiratory system. About ten days after surgery, the patient is discharged, but treatment will continue in the oncology department.
Polypectomy
Rectal polyps are tumor-like formations, mainly of a benign nature. But sometimes their nature changes, and they become malignant tumors. In this case, a radical method of treatment is rectal cancer resection.
In the presence of polyps with symptoms of malignancy, a part of the rectum is excised or it is completely removed. The length of the removed area depends on the degree of damage to the polyp. With the spread of the cancer process to nearby areas of the rectum, the entire affected part is removed. And if metastases appeared, then lymph nodes are also subject to excision.
Types of intestinal compounds after resection
After removing the abnormal part of the intestine, the doctor must connect the remaining ends or apply an anastomosis. Opposite ends of the intestine may vary in diameter, so technical difficulties often arise. Surgeons use three types of compounds:
- End to end is the most physiological and often used way to recreate intestinal integrity.
- Side to side - used to connect the ends when their diameters do not match.
- Side to end - used to connect different parts of the intestine.
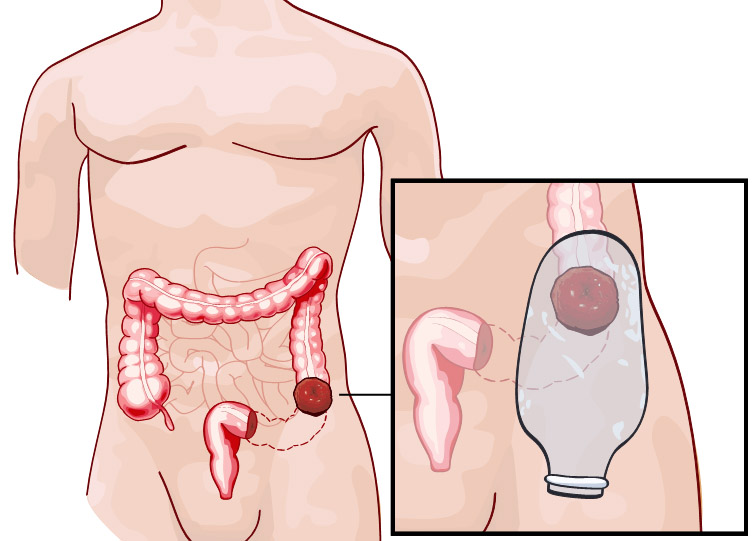
For stitching, use a manual or hardware seam. With the technical impossibility of restoring the intestine or for the quick restoration of its functions, an overlay of the colostomy (outlet) on the anterior abdominal wall is used. With the help of her feces are collected in a special colostomy bag. The temporary colostomy is removed after a few months, and the constant remains until the end of life.
The consequences of rectal resection
The operation to remove part of the rectum sometimes has negative consequences:
- If sterility is impaired in the operating room or instruments, a wound infection occurs. In this case, redness and suppuration of the suture is formed, the patient rises in temperature, chills and weakness are observed.
- The occurrence of internal bleeding. It is dangerous in that it does not appear immediately.
- With intestinal scarring, intestinal obstruction may occur. In this case, a second operation will be required to eliminate it.
- Anastomositis is the occurrence of an inflammatory process at the junction of the ends of the rectum. The causes of inflammation are the body's reaction to suture material, poor adaptation of stitched mucous membranes, tissue injury during surgery. The disease has a chronic, catarrhal or erosive form.
After resection of the rectum, the operated organs continue to function and can be injured by feces. To prevent injuries, the patient must strictly follow the diet recommended by the doctor and exclude physical activity for six months.
Postoperative nutrition
In the postoperative period, it is especially important to follow a special diet so that it does not injure the intestines, does not cause fermentation processes and diarrhea. In the first day after surgery, the patient is starving, the necessary vitamins and minerals are administered intravenously. Within two weeks, dairy products, legumes, raw vegetables and fruits are excluded. Subsequently, the diet does not greatly limit the diet of the operated patient. Sample menu after rectal resection:
- In the morning, drink a glass of boiled clean water. After half an hour, eat oatmeal cooked in water, adding a small amount of walnuts to it, and drink a cup of jelly.
- After three hours, use applesauce for a snack.
- For lunch, soup with buckwheat and fish dumplings, and tea brewed with herbs are suitable.
- An afternoon snack consists of a handful of crackers and a glass of kefir.
- For dinner, you can eat rice porridge, steamed chicken meatballs and compote.
For cooking, there are many different recipes, so that the food is varied, you can use them.
Colorectal Cancer Prevention
In order to prevent colon cancer, you should lead a healthy lifestyle, breathe fresh, clean air, drink quality water, eat more plant-based foods and limit the use of animal fats. An important factor is secondary prevention, timely detection of polyps and their removal. There is a high probability of detecting cancer cells in a polyp, the value of which is more than five centimeters. The polyp develops very slowly over 10 years. This time is used for a preventive examination, which begins to be carried out from the age of fifty in people who do not have risk factors for developing colon cancer. For those who are predisposed to the occurrence of cancerous tumors, preventive measures begin ten years earlier. It is important when you see suspicious symptoms in the bowel, immediately consult a doctor and undergo an examination so as not to undergo a rectal resection.