Cardiovascular diseases are sequentially interconnected and gradually aggravate each other's severity. So, atherosclerosis causes ischemic disease, and hypertension - an increase in the left ventricle of the heart. These conditions simultaneously accelerate the development of heart failure, increase the likelihood of developing myocardial infarction or angina pectoris.
Some of the adverse events that lead to the appearance of cardiovascular diseases can be recognized at the age when their correct correction is possible. Therefore, such concepts as left ventricular hypertrophy (LVH) and dilatation should be given special attention, as well as studying the diseases in which they appear, trying to form a prognosis and tactics for their correction.
The concept of hypertrophy and dilatation
Hypertrophy and dilatation are those morphological phenomena that lead to an increase in heart size mainly due to the left ventricle and atrium, less often due to the right ventricle of the heart. Hypertrophy is an increase in the left ventricle of the heart, a thickening of the myocardium, especially the interventricular septum and posterior wall, caused by physical training or diseases that violate intracardiac hemodynamics (defects and hypertrophic cardiomyopathy) and afterload (hypertension). LVH is accompanied by an increase in stroke volume and an acceleration of contraction, allowing more blood to be pushed into the receiving vessels under higher pressure.
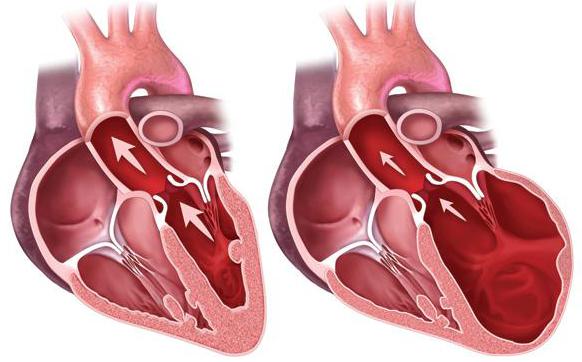
Dilation is a stretching and thinning of the walls of the myocardium caused by a deterioration in the nutrition of the heart muscle and their inability to withstand the actual blood pressure inside the cavities, which is accompanied by an increase in LV filling and a significant decrease in its ejection fraction. This process inevitably follows severe hypertrophy due to its decompensation or appears primarily as a result of the development of dilated cardiomyopathy.
Identification of an increase in LV size
An increase in the left ventricle of the heart, the causes of which will be indicated below, can be determined by a simple examination of the patient, during echocardiography, ECG or x-ray diagnostics. Often this becomes an asymptomatic diagnostic finding when examining a patient for other reasons.
Signs of hypertrophy will be an increase in the percussion borders of the heart, a shift of the apical impulse to the left and an expansion of its area, which can be determined by a medical examination. During dilatation, the percussion borders are also expanded, however, the apical impulse spilled and weak, may not be determined at all in patients with overweight. So you can suspect an increase in the left ventricle of the heart (what is it from a medical point of view - read below).
Electro and echocardiography
When performing an ECG, a functional diagnosis physician often gives an opinion on hypertrophy based on the calculation of standard indices based on measuring the voltage of the R and S teeth in the chest leads. Dilatation of cavities using an ECG is determined indirectly on the basis of systolic overload, which cannot reliably indicate an increase in the left ventricle of the heart. Treatment only on the basis of the ECG in this case is impossible to prescribe, if we are not talking about concomitant arrhythmias.
ECG in detecting structural pathologies of the heart is only one of the reasons to prescribe an ultrasound of the heart, which will make it possible to measure the size of the organ cavities and determine the thickness of the myocardium. With dilatation, the heart is dilated along with a decrease in wall thickness, and with hypertrophy, the myocardium thickens, often even leading to a decrease in the ventricular cavity.
X-ray diagnosis
Hypertrophy or dilatation, especially pronounced, can be determined by x-ray examination. Fluorography or radiography allows you to see the configuration of the heart. With hypertrophy due to aortic valve disease, a corresponding configuration is observed with expansion of the left ventricle and the usual size of the atrium.
If the mitral valve is afflicted, the configuration is very different: it shows enlargement of the atria with normal or only slightly increased LV. Hypertrophic cardiomyopathy can even be marked by a specific configuration, which, due to its large size, is called a "bovine heart". With dilated cardiomyopathy, an X-ray image shows signs of an aortic and mitral configuration, often associated with an expansion of the right borders of the heart.
The role of LVH and dilatation in the development of heart failure
The relationship between hypertrophy, dilatation, acute coronary syndrome, and congestive heart failure is straightforward and easy to track. As a result of prolonged hypertension or the presence of an uncorrected defect, the normal myocardium hypertrophies and compensates for the effect of these diseases for a long time. With a further increase in the left ventricle of the heart and atria, transient, and then permanent ischemia develops, which gradually leads to the death of myocardial cells. The result is a weakening of the walls of the heart, which is most pronounced in the left ventricle, causing pulmonary hypertension and first left ventricular, and then total heart failure with stagnation in the circulatory circulation.
Causes of LVH and dilatation
All known causes of an increase in the left ventricle of the heart must be clearly differentiated as factors of development of either hypertrophy or dilatation. These morphological changes in the structure of the heart muscle have a different origin, but the same outcome, which depends on the degree of myocardial transformation. Among the causes of left ventricular hypertrophy are:
- physical strength and dynamic exercises, fitness;
- arterial hypertension;
- hypertrophic cardiomyopathy;
- compensated aortic stenosis or aortic insufficiency;
- compensated heart defects.
The causes of dilatation of the heart are much smaller, and they should be divided into primary and secondary. Primary include hereditary dilated cardiomyopathy, a disease associated with a defect in the structural proteins of muscle cells. For this reason, the myocardial wall does not withstand the blood pressure inside the cavities of the heart, due to which it gradually stretches and becomes thinner. Secondary causes of dilatation include decompensation of congenital and acquired defects, acquired dilated cardiomyopathy (alcoholic, toxic or radiation).
Degrees of hypertrophy
The above is an explanation of the concept of what means an increase in the left ventricle of the heart, however, how it should be interpreted should be examined in more detail. If, during dilatation, the prognosis of heart failure with a drop in the ejection fraction is inevitable, then with LVH this can be avoided in most situations. Therefore, to formulate a prognosis, it is proposed to more fully evaluate the extent of hypertrophy by echocardiographic criteria.
The normal LV wall thickness in women is 0.6 - 0.9 cm, and in men 0.6 - 1.0 cm in the area of the interventricular septum (MJP) and the posterior wall of the left ventricle (LVL).
With a mild degree of hypertrophy in women, there is a thickening of the VLHF and MJP to 1.0 - 1.2 cm, with an average of 1.3 - 1.5 cm, and with severe - more than 1.5 cm.
In men, a mild degree of LVH is observed with a thickness of MJP and ZLZH in the range of 1.1 - 1.3 cm, an average degree of 1.4 - 1.6 cm, and with a severe one - 1.7 and more.
Physiological hypertrophy
In the framework of sports medicine, there is such a thing as physiological functional hypertrophy, caused by intensive training of the body, myocardium and skeletal muscles. This process allows for a stronger contraction of the heart and expulsion of a larger portion of blood into the receiving arteries, which ensures intensive nutrition of the muscles of the body than in an untrained patient.
Physiological hypertrophy is the more pronounced, the harder the sport, and the more dynamic or static loads it requires. However, what distinguishes it from pathological hypertrophy, it leads to an increase in the ejection fraction of the left ventricle of the heart. That is, a portion of blood that has fallen into the left ventricular cavity is pushed out more fully than in an untrained patient, faster and stronger. If a healthy person has an ejection fraction of about 65-70%, then in an athlete it can be 80-85% or higher.

This is what determines the ability of the heart to overcome intense physical activity. At the same time, physiological LVH rarely goes beyond mild boundaries according to echocardiography, and is also characterized by a rich network of collaterals in the myocardium. Because of this, the risk of developing heart failure in the absence of other more important factors, for example, hypertension, is quite low. In this case, hypertrophy is necessary to increase the fraction of the left ventricle of the heart, and not to overcome the general peripheral vascular resistance, as in the case of hypertonic hypertrophy.
Combined hypertrophy
If the athlete has hypertension, professional training should be discontinued, as LVH will take the form of a pathological rather than compensatory mechanism. The only reason inherent in increasing the ejection fraction of the left ventricle of the heart will now work against increasing exercise tolerance. Myocardial volume will increase, after which the subepicardial sites will begin to experience constant ischemia. This will inevitably lead to the appearance of angina pectoris, will provide an increased risk of early development of myocardial infarction.
LV enlargement treatment
In the debatable question of how to treat an enlargement of the left ventricle of the heart, there is not yet an adequate, unambiguous answer for the reason that this condition is not considered a disease, with the exception of heart defects and dilatation. With hypertension, the main drugs that lower blood pressure are able to prevent the development of LVH. All ACE inhibitors (Enalapril, Lisinopril, Quinapril, Ramipril), angiotensin receptor blockers (Candesartan, Lozartan, Valsartan), diuretics (Indapofon, Hydrochlorothiazide) have this property. , "Furosemide", "Torasemide").
Prevention of LV hypertrophy
The doctor, prescribing a combination of drugs for the treatment of hypertension or heart failure, thereby achieving a slowdown in the development of hypertrophy and dilation. This means that the prevention of hypertrophy is effectively achieved during the pharmacological treatment of hypertension, malformations, acute coronary syndromes and subsequent angina pectoris.
In situations where a patient has a certain heart defect, it is reasonable not to wait for the time of decompensation, when hypertrophy is transformed into dilatation, but to correct the disease surgically. In the case of decompensation of hypertrophic (especially concentric or obstructive) or dilated cardiomyopathy, young patients have a heart transplant or temporary implantation of prosthetic left ventricle.