Fractures of the lower leg require long-term treatment with the immobilization of the damaged leg: a closed fracture of the lower leg without displacement or with a slight displacement of fragments is treated by applying a plaster cast for an average of 2-2.5 months, with an open fracture and with fractures with a longitudinal displacement, there is a need for a longer immobilization after skeletal tension or surgery.
Therapeutic exercises for fracture of the leg should begin from the first days in the absence of pain at the fracture site and in good general condition of the patient. The day after traction is applied, restoration procedures are started in the form of massage and exercises of the intact leg, superficial massage of the thigh of the injured leg and movements in the ankle joint. Fractures of the lower leg are treated more quickly with an early transition to minor active movements in the knee joint (by pulling the load). The tensile stress arising in this case in fragments promotes the activation of regeneration processes. After about 4 weeks, it is possible to bend the knee joint to almost a right angle.
From the moment the plaster cast is applied, they move to the gradual stay of the patient in an upright position. The next day, you can sit in bed, dangling your leg, and also put your foot on the floor without load. On the third day, you are allowed to stand by the bed, holding on to a support (chair or bed frame). At the end of the exercises, you should definitely give the leg an elevated position. The development of proper walking with crutches begin after 4-5 days.
From the first days of walking, you should rely on a plaster cast. This creates the axial load of the damaged limb, necessary for the functional training of bone marrow. Due to the micromotion of the fragments, a quick fusion occurs with the formation of massive corns. In the absence of such a load, consolidation slows down and severe osteoporosis develops.
The goal of physical therapy after a leg fracture at this stage is to switch from a dosed constant load of the sore leg when walking with crutches to constant and full loads, allowing movement without crutches. With an increase in load, one should focus on the appearance of pain: walking should be accompanied by minor pain, in which protective reparative processes are activated, aimed at eliminating the irritant. Excessive pain indicates significant trauma to the corns, which leads to a slowdown in regeneration.
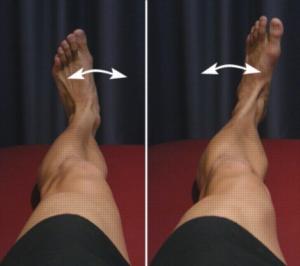
Shin fractures are treated more efficiently when performing special therapeutic exercises (6-8 movements each):
- In the supine position - this is the implementation of the back and plantar flexion of the feet, isometric tension of the muscles of the thigh (up to 5 times for 5 seconds), alternating flexion and extension of the legs in the knee joint when sliding the foot on the bed, alternating abduction and bringing the legs when sliding on the bed grabbing and holding small objects with the toes, circular movements of the feet and simulating walking in bed.
- Lying on the stomach, bend and extend the leg in the knee joint, take the straight leg back and to the side.
- Lying on their side, they take the straight leg to the side and hold it in this position for up to 5 seconds.
- In the sitting position, the toes of the feet are bent and unbent, the medicine ball is rolled back and forth with the fingers, the foot is rolled from heel to toe.

Shin fractures are treated effectively only with the active participation of the patient in recovery activities, one of which is physiotherapy. Only with a clear understanding of the goals and details of rehabilitation treatment can a patient mobilize his will for regular and persistent exercise.