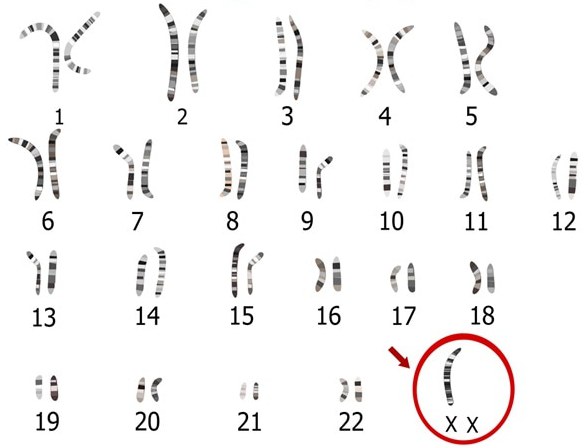
Shereshevsky-Turner Syndrome (also Ulrich-Turner Syndrome) is a genetic disease caused by the complete or partial absence of one X-chromosome in women. Like other chromosomal abnormalities, it is characterized by severe consequences for patients. The karyotype for Turner syndrome is designated as 45, X0.
Genetics
In short, Turner syndrome develops in the case of a complete or partial monosomy of the X chromosome in a woman. In approximately 20% of cases, the disease is associated with mosaicism of the X chromosome - a condition in which in some cells of the female body there are two normal X chromosomes, one of which is inactive, and in other cells one of the sex chromosomes is substantially damaged or completely absent. Sometimes there is a transition of a part of the X chromosome to an autosome (translocation).
In some cases, the syndrome is associated with the appearance of the so-called ring chromosomes or isochromosomes. Ring chromosomes occur when the ends of a chromosome are broken and their long and short shoulders join together to form a ring. Isochromosomes occur when a lost long or short arm of a chromosome is replaced by an identical copy of the other arm.
There have been cases when in patients some cells have only one copy of the X chromosome, while in other cells there is an X chromosome and some material of the Y chromosome. The amount of material on the Y chromosome is not enough to cause the body to develop according to the male type, but its presence is associated with an increased risk of developing a form of cancer known as gonadoblastoma.
More than 90% of pregnancies in the case of a Shereshevsky-Turner syndrome in the fetus result in miscarriage or stillbirth, about 15% of spontaneous abortions are associated with this pathology. However, it is worth noting that this is the only monosomy in the human body, which in some cases is compatible with life: monosomy for any autosome (non-sex chromosome) or the U chromosome inevitably leads to fetal death in the early stages of pregnancy. Appropriate medical care can help relieve symptoms of the disease in children born with Ulrich-Turner syndrome.
Symptoms of the disease are very different in different patients. Most patients are characterized by low growth due to pathologies of the development of the skeleton, a short neck, underdevelopment of secondary sexual characteristics, pathology of the organs of vision and the cardiovascular system, and infertility. Despite this list of symptoms, Turner syndrome is far from the worst genetic pathology - the patients' intellect is generally preserved, and with the right course of treatment, women with such a genetic abnormality can lead a normal lifestyle.
Ulrich-Turner syndrome can be detected before birth using modern diagnostic methods, which will be discussed below. Unlike other genetic diseases, the syndrome is not inherited within families and appears spontaneously (sporadically).
Causes
The causes of Shereshevsky-Turner syndrome are not well understood. It is not known exactly what factors influence the probability of having a baby with this disorder. It has been hypothesized that the risk of the syndrome is affected by exposure of the mother to high doses of ionizing radiation (more than 1 mSv per year). Large-scale studies related to the identification of the causes of Turner syndrome and other chromosomal abnormalities were carried out in the 70s of the last century. The studies were conducted in the Indian state of Kerala, where the background radiation is significantly higher than normal due to the presence of thorium and its decay products in the soil, and in the Chinese province of Guangdong, where the annual equivalent dose is 6.4 mSv. The results showed that increased doses of ionizing radiation increase the risk of having children with Down syndrome and feline scream syndrome. However, there was no increase in the occurrence of Turner syndrome. Today, in many sources you can find information that ionizing radiation affects the risk of developing pathology, but there are no statistics that would confirm this.
There was also no relationship between the age of the mother and the probability of having a baby with this pathology.
Symptoms
For patients with this disease are characteristic: low growth, pathology of the development of the skeleton and secondary sexual characteristics. The disease can affect other organ systems. The presence of Shereshevsky-Turner syndrome does not mean that one patient will have all the possible signs of the disease. The syndrome is characterized by a wide range of symptoms and specific external features. The presence of certain symptoms, their severity and time of manifestation are strictly individual.
Most babies with Turner syndrome are born prematurely and are underweight. In newborns, swelling of the hands and feet is often observed. Many patients in adolescence appear overweight or obese, growth slows down, underdevelopment of the mammary glands and uterus, amenorrhea, chest deformation. Sometimes pathologies such as horseshoe kidney, hypoplasia of the left heart, narrowing of the aorta, and in adulthood - arterial hypertension are found.
Intelligence in patients is usually normal, but there may be difficulties associated with concentration and remembering new material. Some children with Turner syndrome in childhood and adolescence have ADHD - attention deficit disorder and hyperactivity disorder.
Patients have an increased risk of hypothyroidism due to autoimmune thyroiditis. Some women with Turner syndrome have gluten intolerance (celiac disease).
Possible symptoms of the disease also include: high palate, low hairline, underdevelopment of the lower jaw. There are pathologies of the organs of vision and the urinary system.
Prenatal diagnosis
It is no secret that modern diagnostic methods can detect the majority of genetic abnormalities of the fetus long before birth. One such procedure, non-invasive prenatal testing (screening for extracellular DNA of the fetus in the mother’s blood), can be performed from the end of the first trimester of pregnancy.
The advantage of this procedure is that it is not at all dangerous for the mother and fetus. In addition to Turner’s syndrome, extracellular DNA screening reveals aneuploidy such as Patau syndrome (trisomy on the 13th chromosome), Edwards syndrome (trisomy on the 18th chromosome), Down syndrome (trisomy on the 21st chromosome), trisomy on the X chromosome , Klinefelter syndrome, Martin-Bell syndrome.
Using ultrasound, you can identify abnormalities in the development of the kidneys and heart - they relate to possible symptoms of the disease.
The syndrome can be detected by amniocentesis or a chorionic biopsy. Both of these procedures are invasive and have contraindications. Their advantages include high accuracy of the result.
Diagnosis in childhood and adolescence
The presence of Shereshevsky-Turner syndrome does not always come out to detect before childbirth. Many women whose pregnancy is proceeding normally do not consider it necessary to resort to prenatal diagnosis of fetal genetic abnormalities, some refuse it because of contraindications or fear of side effects. Then the birth of a child with a chromosomal abnormality becomes a surprise to them.
In some cases, Turner syndrome in children can be diagnosed immediately after birth, while mild forms of the disease often go unnoticed by specialists and parents of the child until the onset of the teenage period. It happens that the first three to four years of life, the child develops normally. After this, growth sharply slows down, and lagging behind peers in physical development becomes noticeable. In elementary school, learning difficulties arise because of the inability to concentrate. It is especially difficult for children with Turner syndrome to have sciences that require a high concentration of attention and spatial thinking.
By the end of the puberty, girls with this genetic abnormality are much lower than their parents (the average height of women with Ulrich-Turner syndrome is 145 cm), skeletal abnormalities and other symptoms of pathology are noticeable. To verify the presence of the disease in the child, you should consult a specialist who will suggest karyotyping, a diagnostic procedure that allows you to identify chromosomal abnormalities in the genome. This procedure is absolutely safe, painless and has no contraindications. During karyotyping, the researcher takes several venous blood cubes for analysis and examines the mitotic cycle of the leukocytes isolated from there.
Treatment
At the moment, there are no procedures or drugs that have allowed the treatment of Turner syndrome. Perhaps, in the future, gene therapy will allow to restore the lost X chromosome during embryogenesis, but so far such procedures remain beyond the scope of what is possible. Treatment of Shereshevsky-Turner syndrome remains symptomatic. To correct short stature, hormonal preparations containing somatotropin are prescribed, which are taken before and during the puberty. The sooner somatotropic therapy begins, the more effective it will be.
For more than seventy years, estrogen replacement therapy has been used for normal development in patients with secondary sexual characteristics, it is prescribed at the age of 12-14 years. To maintain a normal balance of hormones in the body, most women require estrogen and progesterone before menopause.
Estrogen is also key to maintaining bone integrity and the normal functioning of body tissues. Women with Shereshevsky-Turner syndrome without estrogen administration increase the risk of osteoporosis and heart disease.
With hypothyroidism, patients are prescribed the introduction of thyroid hormones.
If patients have diabetes, they need to constantly monitor the level of insulin in their blood and adhere to a diet.
If a woman with Ulric-Turner syndrome has a horseshoe-shaped kidney or malformations of the urinary system, a nephrologist and a urologist should be consulted.
Forecast
The prognosis, as with any genetic pathology, depends on the severity of the symptoms. Many women who have undergone hormonal therapy live a full life. They have a normal level of intelligence and learning ability.
Almost all patients with Turner syndrome are not able to have children. Medicine knows cases when such women could become pregnant on their own, but this is very rare. Most patients solve this problem with the help of artificial insemination.
It should be remembered that women with Turner syndrome have an increased risk of complications during pregnancy. They need constant monitoring by a gynecologist and therapist.
Of course, those who were diagnosed with Turner Syndrome had a difficult fate. A photo of a young woman suffering from this disease is presented below.
Prevalence
Ulrich-Turner syndrome can not be called a rare disease. Its frequency ranges from 1: 2000 to 1: 5000 in newborn girls, and given the fact that most pregnancies with this syndrome end in a miscarriage or spontaneous abortion, we can say that the incidence of the disease is much higher.
No racial or ethnic factors were identified that would affect the frequency of birth of children with Turner syndrome.
Discovery story
The first to describe this disease was independently described by the Russian endocrinologist Nikolai Shereshevsky in 1925 and the American endocrinologist Henry Turner in 1938. They studied the main symptoms of the pathology, but did not assume that the disease they discovered was associated with a chromosomal abnormality. The German scientist Ulrich also contributed to the study of the disease. In 1930, he described a clinical case in which an 8-year-old patient had no secondary sexual characteristics, low growth, micrognathia (underdevelopment of the upper jaw). In European literature, this chromosomal abnormality is often called Ulrich-Turner syndrome or simply Ulrich syndrome.
The first publication about a woman with a karyotype of Shereshevsky-Turner syndrome belonged to the British physiologist Charles Ford. It was he who determined that the cause of the syndrome is monosomy on the X chromosome.
Medical curiosity
There are two more diseases that are sometimes abbreviated as Turner syndromes. These pathologies were discovered and described by the namesake of the American endocrinologist Henry Turner, hence the confusion with the names. These are the May-Turner and Personage-Turner syndromes. Both of these diseases are in no way associated with the X chromosome monosomy described above, and are not even hereditary diseases.
The first description of May-Turner syndrome appeared in 1957. Pathology is manifested by a violation of the outflow of venous blood from the left lower limb and pelvic organs, as a result of which patients suffer from constant pain in the left leg and pelvic region. In the later stages of the disease, venography shows deep vein thrombosis. The syndrome is difficult to diagnose, especially in the early stages, as it is asymptomatic at first. May-Turner syndrome usually begins in adolescence, is more common in men than in women.
Ultrasound of the iliac veins of the pelvis is used as the main diagnostic procedure. In the case of a disease, the left common iliac vein in diameter is much larger than normal. Magnetic resonance angiography of the iliac veins with contrast is used to confirm the diagnosis. In the later stages of the disease, treatment is performed surgically. Often prescribed medications to restore normal blood flow.
Personage-Turner syndrome is rare in clinical practice and its causes have not yet been precisely established. The first signal about the presence of the disease is a sharp causeless pain in the shoulder or arm, less often in both hands at the same time. Many people who first showed this pathology do not consider it necessary to seek help from a specialist, hoping that the symptoms disappear on their own.
The pain may not go away for several days, sometimes several weeks. The pain intensifies with movement and weakens if the limb is at rest. Many patients stop developing the arm, which is why muscular dystrophy develops over time. In most people, the disease goes away over time without any intervention. Sometimes you need to take strong analgesics. The causes of Personage-Turner syndrome are of great interest to physicians, but have not yet been studied. The prevalence of the disease is also not known.